Gum Disease and Your Overall Health: What the Research Actually Links

When patients hear “gum disease,” most picture a dental problem — something that affects their teeth and, at worst, costs them a tooth eventually. What surprises most people is how much research now connects the health of your gums to conditions well outside your mouth: heart disease, diabetes, pregnancy complications, and more. None of this is fringe science anymore. Major medical bodies, including the American Heart Association, have issued formal statements on it. Let me walk through what the research actually shows, what it doesn’t prove, and what it should realistically change about how you think about your gums.
What gum disease actually is
Gum disease exists on a spectrum. Gingivitis is the early, reversible stage — inflammation confined to the gum tissue, usually showing up as redness, swelling, or bleeding when you brush. Left untreated, gingivitis can progress to periodontitis, a more advanced form where the inflammation has spread to the structures that actually anchor your teeth — the ligament and bone underneath the gumline. This is a chronic inflammatory condition, and it’s far more common than most people realize: it’s estimated to affect roughly 40% or more of U.S. adults over 30, with severe cases affecting around 1 in 10 people globally.
That word — inflammatory — is the thread connecting everything below. Periodontitis isn’t just a local infection sitting quietly in your gums. It’s a source of ongoing, low-grade inflammation and a route for bacteria to enter your bloodstream, and both of those things have effects that reach well beyond your mouth.
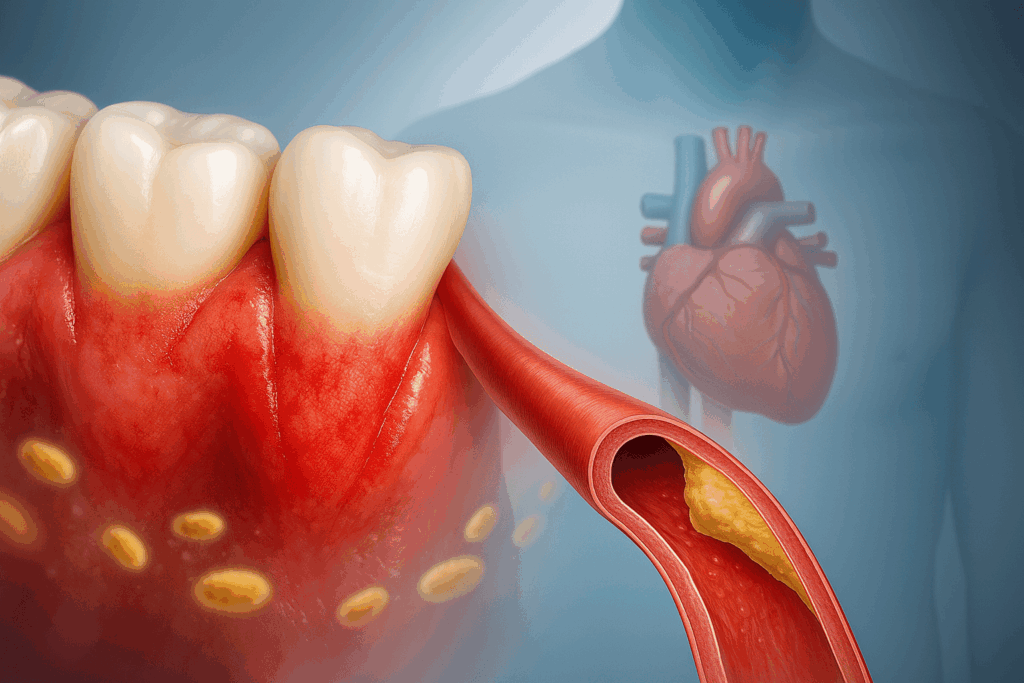
The heart disease connection
In December 2025, the American Heart Association released an updated scientific statement reviewing the evidence linking periodontal disease to atherosclerotic cardiovascular disease, the condition responsible for heart attacks and most strokes. The statement synthesized a large and growing body of research showing associations between gum disease and coronary artery disease, stroke, peripheral artery disease, and cardiovascular death, along with measurable changes in blood vessels themselves, like increased arterial stiffness and thickening of the carotid artery wall.
Two proposed mechanisms explain why: a direct pathway, where oral bacteria enter the bloodstream and contribute to vascular infection and inflammation, and an indirect pathway, where the chronic inflammation from ongoing gum disease raises systemic inflammatory markers already known to drive cardiovascular risk. Notably, the AHA statement was careful to say that periodontal disease and cardiovascular disease share several risk factors — age, smoking, obesity — but that emerging data suggests an association independent of those shared factors as well.
Did You Know
Research cited in the American Heart Association’s 2025 statement found that more frequent tooth brushing was associated with meaningfully lower 10-year cardiovascular risk — 7.35% for people brushing three or more times daily versus 13.7% for those brushing once a day or less — alongside lower levels of inflammatory markers linked to heart disease.
What this doesn’t mean: the AHA statement is explicit that no direct causal link has been established, and that it isn’t yet proven that treating gum disease prevents heart attacks or strokes. What it does mean is that gum health is now considered a legitimate factor worth discussing as part of overall cardiovascular risk, not an unrelated body part.
How researchers are trying to prove causation, not just correlation. One detail in the AHA’s updated statement is worth understanding, because it shows how seriously this question is being taken: the review incorporated findings from Mendelian randomization studies, a research method that uses genetic variants associated with periodontal disease to test whether the relationship with cardiovascular disease behaves the way a true causal relationship would, rather than simply reflecting shared risk factors like smoking or age. This kind of study design is specifically built to get closer to causation than a standard observational study can, and its inclusion signals that researchers are actively working to answer the causation question rather than treating the association as settled.
A note on existing heart conditions and dental visits
If you have certain existing heart conditions — a prosthetic heart valve, a history of infective endocarditis, or specific congenital heart defects — your cardiologist may recommend antibiotic prophylaxis before certain dental procedures, a separate and well-established precaution against a different risk: bacteria entering the bloodstream during a procedure settling on already-vulnerable heart tissue. This isn’t related to the broader gum disease research discussed above, but it’s worth mentioning in the same conversation, since both point to the same underlying reality — your dentist and your cardiologist are managing overlapping, not separate, territory. If you have a significant cardiac history, make sure your dental team knows about it before any invasive treatment.
The diabetes connection
This is the most well-established of the links discussed here, and it runs in both directions. A large meta-analysis pooling data from over 700,000 participants across multiple cohort studies found that people with periodontitis had about a 26% higher risk of developing diabetes than people without it, and separately, people with diabetes had about a 24% higher risk of developing periodontitis than people without diabetes. Diabetes impairs the body’s ability to fight the bacterial infection driving gum disease, while the chronic inflammation from gum disease makes blood sugar control measurably harder — a two-way cycle where each condition tends to make the other worse.
This relationship is well-established enough that periodontitis is sometimes referred to in the research literature as a complication of diabetes in its own right, alongside more commonly recognized ones like nerve damage or kidney disease. It also means the reverse is genuinely actionable: clinical trials have found that treating gum disease in patients with diabetes can measurably improve their blood sugar control, an effect that’s rare to see from a dental treatment reaching into an entirely different area of medicine.
Worth Knowing
If you have diabetes, gum disease isn’t just a separate condition to manage alongside it — the two influence each other directly. Treating active gum disease has been shown in clinical trials to measurably improve blood sugar control, which is part of why dental visits are considered a meaningful part of diabetes management, not a separate concern.
The pregnancy connection
Hormonal changes during pregnancy — particularly elevated progesterone and estrogen — increase blood flow to the gums and make them more reactive to the bacteria already present in plaque, which is why gum inflammation is so common during pregnancy even in women with otherwise good oral hygiene. Beyond the discomfort of pregnancy gingivitis itself, a systematic review of multiple studies found periodontal disease associated with an increased risk of preterm birth and low birth weight, with individual studies reporting the risk elevated by roughly two to four times in mothers with periodontal disease compared to those without.
The proposed mechanism involves the same inflammatory pathway seen elsewhere on this list: periodontal bacteria and the inflammatory compounds they trigger can reach the uterine environment, and elevated inflammatory markers are independently associated with early labor. This is a major reason dental care during pregnancy isn’t just safe but actively recommended — treating gum disease during pregnancy is considered both effective and appropriate at any stage, not something to postpone until after delivery. If you’re pregnant and notice your gums bleeding more than usual, that’s worth mentioning at your next visit rather than assuming it’s simply an unavoidable part of pregnancy to wait out.
The respiratory connection
Less widely known, but well documented particularly in older adults: bacteria from the mouth can be aspirated into the lungs, and in people with reduced immune function or swallowing difficulties, this is an established contributor to pneumonia risk, especially in hospital and long-term care settings. This is part of why oral hygiene protocols are increasingly built into medical care for hospitalized and elderly patients, not treated as a separate concern from their general health.
Other associations worth knowing about
Beyond the conditions discussed in depth above, gum disease has also been studied in connection with rheumatoid arthritis, where shared inflammatory pathways and some overlapping bacterial triggers have researchers investigating whether treating one condition might meaningfully affect the other. It’s also been examined alongside chronic kidney disease and, as covered in a separate piece on this blog, emerging cancer research. None of these associations are as extensively documented as the heart disease and diabetes connections, but they follow the same underlying logic: a chronic inflammatory condition in one part of the body rarely stays perfectly contained to that location.
Why one condition in your gums connects to all of this
Zooming out, the pattern across every connection above is the same one: gum disease is a chronic source of both bacteria entering circulation and ongoing low-grade inflammation, and the body’s inflammatory response doesn’t stay neatly contained to the tissue where it started. Chronic inflammation is already an established contributor to cardiovascular disease, insulin resistance, and complications in pregnancy independent of gum disease specifically — periodontitis is simply one significant, common, and treatable source of that inflammation that often goes unaddressed because it’s painless in its early stages.
What the evidence actually supports, and what it doesn’t
It’s worth being precise here, the same way it’s worth being precise about any research connecting the mouth to the rest of the body: most of these findings are strong associations, not proof of direct causation, and the major statements from bodies like the AHA are explicit about that distinction. What is well-supported is that gum disease is a modifiable source of chronic inflammation, that it’s extremely common, and that treating it is a low-risk, high-value intervention regardless of whether every causal question has been fully answered yet. You don’t need certainty about causation to make addressing an inflamed, bleeding, infected area of your body a reasonable priority.
| Condition | Strength of evidence | Proposed mechanism | What to do |
|---|---|---|---|
| Heart disease | Strong association; causation not yet proven AHA statement, 2025 |
Bacteria entering the bloodstream; systemic inflammation | Treat gum disease; mention cardiac history to your dentist |
| Diabetes | Well-established, bidirectional Strongest link on this list |
Impaired infection control; inflammation affecting blood sugar | Treat gum disease as part of diabetes management, not separately |
| Pregnancy outcomes | Consistent association across multiple studies | Inflammatory compounds reaching the uterine environment | Keep up with dental care during pregnancy; don’t postpone treatment |
| Respiratory disease | Documented mainly in older or immunocompromised adults Higher-risk groups |
Aspiration of oral bacteria into the lungs | Prioritize oral hygiene in elderly or hospitalized care settings |
What this actually means for your care
Treat gum disease as more than a dental inconvenience. If you’ve been told you have gingivitis or periodontitis, that’s worth taking seriously beyond concern for your teeth, particularly if you also have diabetes, cardiovascular risk factors, or are pregnant.
Don’t skip your periodontal evaluations if you have diabetes or heart disease. These conditions make coordinated dental and medical care more valuable, not less — ask your dentist and physician to be aware of both sides of the picture.
If you’re pregnant, keep up with dental care rather than postponing it. Routine cleanings and treatment for gum disease are considered safe and appropriate during pregnancy, and addressing gum inflammation is one of the more actionable steps available to you during this time.
Brushing and flossing consistency isn’t just about cavities. The inflammation reduction that comes from good daily oral hygiene is part of what’s driving the associations described above — consistent home care is doing more systemic work than most people give it credit for.

The bottom line
The research connecting gum disease to heart disease, diabetes, pregnancy outcomes, and respiratory health has moved well past speculation — it’s now reflected in formal statements from major medical organizations, even as researchers continue working out exactly how much of the relationship is causal versus associative. What doesn’t require any more research to act on is this: gum disease is common, it’s largely preventable, it’s treatable, and treating it is one of the more genuinely high-value things you can do for your health beyond your smile. If it’s been a while since your gums were evaluated, a periodontal evaluation is a reasonable thing to prioritize regardless of which specific study eventually gets confirmed — the underlying advice doesn’t really change either way.

Dr. Elizabeth Wakim, DDS, is the founder of Enhanced Wellness. She’s a compassionate and highly-regarded dentist with her own practice in Washington, Pennsylvania, known for providing modern, comprehensive dental care, botox and facial aesthetics with a focus on patient comfort and anxiety reduction, serving general, cosmetic, and pediatric dentistry needs.